Disengagement proposals by the Centers for Disease Control and Prevention (CDC) for those presented to COVID-19 have changed a few times somewhat recently for both the general population and medical care experts. A ton of variables go into the estimation: staffing deficiencies at medical clinics, exactly the amount of a danger Omicron postures, immunization and sponsor status. It tends to be hard to follow, yet Sharon Ward-Fore, MS, MT(ASCP), CIC, FAPIC, an individual from Infection Control Today®’s Editorial Advisory Board clarifies how disease preventionists (IPs) can best assistance their medical care associates follow the proposals. There’s a great deal of dissatisfaction about the pandemic, however Ward-Fore says that “we should begin to zero in on those individuals who know and feel that, ethically, they need to make the best decision, and the proper thing is to appear and do whatever they can to help. Medical care does that. IPs do that. IPs assist with reinforcing medical care staff by supporting them.”
Contamination Control Today®: The Centers for Disease Control and Prevention (CDC) has changed proposals for when medical care laborers who’ve been presented to COVID-19 can return to work a few times somewhat recently or something like that. Where does that stand now?
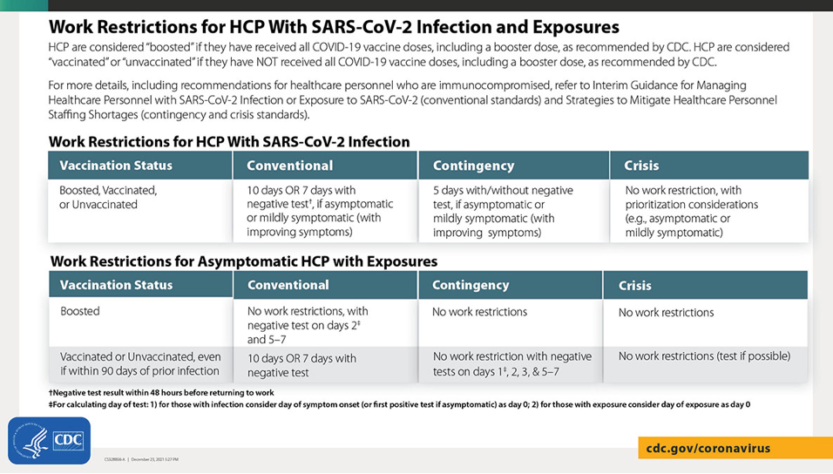
Sharon Ward-Fore, MS, MT(ASCP), CIC, FAPIC: I’m very confounded as well. Yet, I’m trusting that medical services laborers will allude to the CDC site, which was refreshed on 12-23-21, where there’s a great table that clarifies all that you recently said, yet in an outline structure. At the point when I read through what had been composed, I was befuddled. However, when I take a gander at this, it kind of explains things. There’s a table on inoculation status, and afterward they separate it to ordinary, possibility, and emergency staffing, which I think will help explain for a great deal of cases. For instance, for work limitations for medical services laborers with a disease—and as you said, assuming that they’re helped, inoculated, or unvaccinated—the ordinary system is by and large what you said: 10 days or seven days with a negative test, if asymptomatic or somewhat suggestive with further developing indications. That is the ordinary proposal for assuming you have a typical labor force. Assuming that you’re presently on a possibility labor force, they say five days with or without a negative test. In the event that asymptomatic, or somewhat suggestive with further developing manifestations. And afterward they continue to a real emergency standard, which is no work limitations with prioritization contemplations, asymptomatic or somewhat indicative. To give the CDC a little credit this has truly been a moving objective with such countless various subtleties that I think assuming we give this diagram, it ought to explain a ton of things. Furthermore on the off chance that you have a customary labor force, obviously, you know, you can do what’s to the greatest advantage of your staff and patients. Also recollect, these are suggestions. Believe that with some hesitancy. You generally need to be really severe as this, yet you can be significantly stricter, if possible. Presently I know there are a few organizations that are following the traditional technique with 10 days or seven days and a negative test. In any case, presently they’re additionally seeing, “Indeed, how might we forestall evening manage this in any case?” And for those offices that have enough PPE, they’re suggesting that their medical care laborers all wear N95s. What’s more we realize that this is an airborne respiratory infection. What’s more the main way we shield ourselves from airborne particles is with a N95. I feel that is a decent positive development. Assuming you have how much N95s to have the option to permit that.